The Assess and Classify chart will help you identify ear problems caused by ear infection. You should ask about ear problems for every sick child who is brought to your health post.
When you assess a child you will be looking for the following signs:
Box 13.1 is from the 'Assess' column in the Assess and Classify chart that tells you how to assess a child for ear problems.
ASK: Does the child have an ear problem?
| IF YES, ASK: | LOOK AND FEEL: |
|---|---|
|
∙ Is there ear pain? ∙ Is there ear discharge? If yes, for how long? |
∙ Look for pus draining from the ear ∙ Feel for tender swelling behind the ear |
If the mother answers no, you do not need to assess the child for ear problems. Your next question in this case would be whether the child has a throat infection (you will learn about throat infections in Section 13.2 below).
If the mother answers yes, ask the next question:
If the mother is not sure that the child has ear pain, ask if the child has been irritable and rubbing his ear. Whether the answer is yes or no you should ask the next question.
When asking about ear discharge, use words the mother understands. For example, 'Is there any fluid that looks like pus coming out from the ears?' If the child has had ear discharge, ask the mother for how long.
Look inside the child's ear to see if pus is draining from the ear. Pus is usually white, creamy or light green and may have an offensive smell.
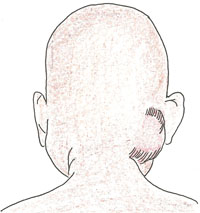
Feel behind both ears. Compare them and decide if there is tender swelling of the mastoid bone. In infants, the swelling may be above the ear.
Both tenderness and swelling must be present to classify mastoiditis, a deep infection in the mastoid bone. You can see an illustration of this in Figure 13.1.
How can you find out whether a sick child brought to your health post has ear problems?
You could ask the mother whether the child has been irritable and rubbing his ear, which suggests it might be painful. You would ask her whether there has been any fluid coming from the child's ear and for how long this has been happening.