The purpose of airway assessment is to identify possible difficulty with laryngoscopy (and hence tracheal intubation), mask ventilation, or creation of a surgical (percutaneous) airway. Air way assessment is accomplished by history, physical examination and radiologic examination in specific cases.
The patient's airway history should be evaluated to determine whether there are any medical, surgical, or anesthetic factors that have implications for airway management. Preoperative assessment of the airway begins with careful questioning of the patient about their medical history.
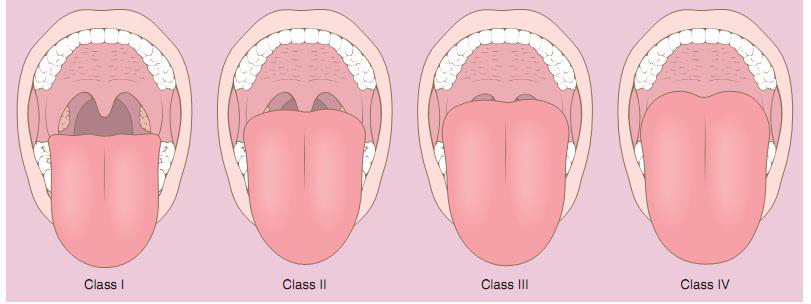
4.1.2.1 Oropharyngeal space: Malampati proposed a classification system (Malampatti score) to correlate the oropharyngeal space with the ease of direct laryngoscopy and tracheal intubation (Figure 4.1). With the observer at eye level, the patient holds the head in a neutral position, opens the mouth maximally, and protrudes the tongue without phonating. The airway is classified according to the visible structures. Class III may be difficult to intubate and class IV is most likely to be difficult.
Class II: The soft palate, fauces, and uvula are visible.C
Class III: The soft palate and base of the uvula are visible.
Class IV: The soft palate is not visible. There is a correlation between the Malampatti score, what can be seen on direct laryngoscopy, and the ease of intubation (Figure 4.2). >
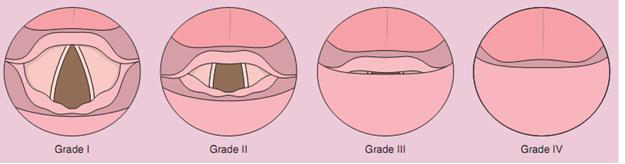
Grade I: Most of the glottis is visible.
Grade II: Only the posterior portion of the glottis is visible.
Grade III: The epiglottis, but no part of the glottis, can be seen.
Grade IV: Hard and soft palate not seen
4.1.2.2The Inter-incisor gap: the size and position of the maxillary and mandibular teeth and the conformation of the palate should be assessed. An inter-incisor gap of less than 3 to 4.5 cm correlates with difficulty achieving a line of view on direct laryngoscopy. Maxillary prominence or a receding mandible also correlates with a poor laryngoscopic view. Overbite, a condition where the front teeth overlap the lower teeth excessively, results in a reduction in the effective inter-incisor gap when the patient's head and neck are optimally positioned for direct laryngoscopy.
4.1.2.3 Mandibular length: It is the distance from symphysis to angle of jaw. The normal distance is 9cm. Micrognathia (small jaw) limits the pharyngeal space (tongue positioned more posterior) and the space in which the soft tissues are going to be displaced during direct laryngoscopy. This causes the glottic structures to be anterior to the line of vision during direct laryngoscopy. Various genetic syndromes and acquired disease states limit the pharyngeal space and are difficult to assess on physical examination.
4.1.2.4 Atlano-occipital extension/ Neck mobility:Head elevation and neck flexion bring the pharyngeal and laryngeal axes into line (Figure 4.3). Extension of head at atlanto-occipital joint aligns the oral axis with the other two axes (the laryngeal and pharyngeal axes).
| Figure 4.3 Schematic diagram showing alignment of the oral axis (OA), pharyngeal axis (PA), and laryngeal axis (LA) in four different head positions. |
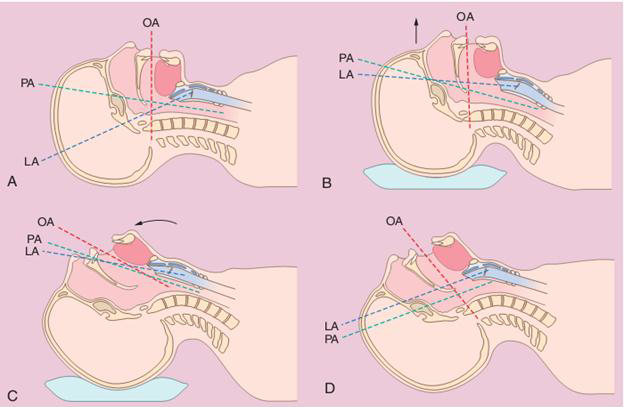 A- The head is in a neutral position with a marked degree of nonalignment of the OA, PA, and LA. B- The head is resting on a large pad that flexes the neck on the chest and the LA with the PA C- ,The head is resting on a pad (which flexes the neck on the chest) with concomitant extension of the head on the neck, which brings all three axes into alignment (sniffing position). D- Extension of the head on the neck without concomitant elevation of the head. |
4.1.2.6 The submandibular space: There are different factors that affect the submandibular space and visualization of the larynx (Table 4.1). Submandibular space is the area into which the soft tissues of the pharynx must be displaced to obtain a line of vision during direct laryngoscopy. Anything that limits the size of this space or compliance of the tissue will decrease the amount of anterior displacement that can be achieved. Ludwig's angina (cellulitis of the mouth and some parts of the neck which causes the neck to swell and may obstruct the airway), tumors, radiation scarring, burns, and previous neck surgery are conditions that can decrease submandibular compliance.
| Table 4: 1 Physical features that may complicate intubation include the following |
|