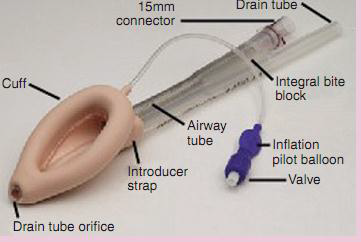
Figure 5:13:LMA
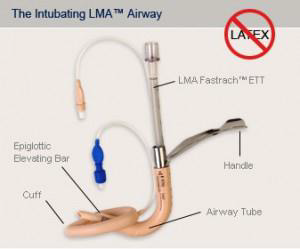
Fig 5.14: intubating LMA
It is an alternative to mask ventilation during a general anesthetic (Figure 5.13 and 5.14). The laryngeal mask airway does not protect against aspiration of gastric contents.
The laryngeal mask airway should not be used in the following situations:
Complications related to the use of the laryngeal mask airway include:
| LMA size | Patient size and wright | Maximum air for cuff inflation |
|---|---|---|
| 1 | Neonates and infants (up to 5 kg) | 4 ml |
| 2 | Infants and children (10-20 kg) | 10 ml |
| 3 | Children (30-50 kg) | 20 ml |
| 4 | Small Adults (50-70 kg) | 30 ml |
| 5 | Adults (70-100 kg) | 40ml |
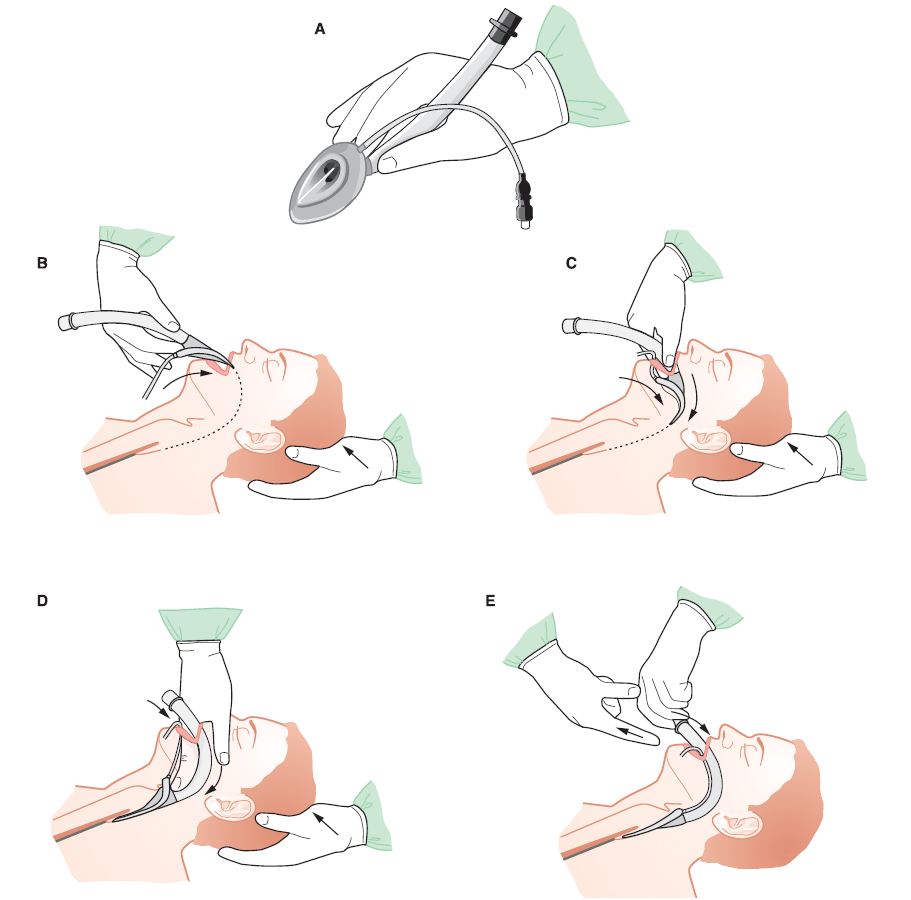
A. The LMA is held by the index finger and the thumb facing the bowl of LMA caudally toward the larynx. The index finger is positioned between the shaft of the LMA and the deflated cuff. The occiput is stabilized with left hand.
B. The deflated and lubricated LMA is placed into the open mouth pressed against the hard palate.
C. The LMA is advanced behind the tongue and into the oropharynx using the index finger.
D. The LMA is pushed further down deep into the hypopharynx using the tip of the index finger.
E. The index finger is removed. The LMA is pushed farther down to its final position by holding the tube of the LMA with the left hand. Without holding the tube of the LMA, the cuff is inflated with the recommended volume of air. The LMA may protrude slightly on inflation of the cuff. Final position of the LMA with cuff inflated. A bite block made of sponges is placed between molars and taped to the LMA tube to prevent patient biting.
After surgery leave the laryngeal mask in place until the patient responds to verbal commands. The cuff does not require to be deflated before removal. Patients, as they awaken, can be encouraged to remove their own laryngeal masks.