A difficult airway is defined as the clinical situation in which a conventionally trained anesthetist experiences difficulty with face mask ventilation, difficulty with tracheal intubation, or both. The difficult airway represents a complex interaction between patient factors, the clinical setting, and the skills of the practitioner.
It is not possible for the anesthetist to provide adequate face mask ventilation (bag mask ventilation). It is inability maintain oxygen saturation (SaO2) >90% using 100% oxygen and positive pressure mask ventilation in a patient whose SaO2 was >90% before clinician intervention. Difficulty may be due to one or more of the following problems: inadequate mask seal, excessive gas leak, or excessive resistance to the ingress or egress of gas. Signs of inadequate face mask ventilation include (but are not limited to) absent or inadequate chest movement, absent or inadequate breath sounds, auscultatory signs of severe obstruction, cyanosis, gastric air entry or dilatation, decreasing or inadequate oxygen saturation (SpO2), absent or inadequate exhaled carbon dioxide and hemodynamic changes associated with hypoxemia or hypercarbia (e.g., hypertension, tachycardia, arrhythmia).
A response to difficult bag mask ventilation
It is not possible to visualize any portion of the vocal cords after multiple attempts at conventional laryngoscopy. Difficult tracheal intubation is tracheal intubation requires multiple attempts (greater than three), in the presence or absence of tracheal pathology.
7.2.2.1 The danger of multiple intubation attempts: Multiple intubation attempts (defined as three or more) have been associated with significant complications, and ultimately poor patient out-comes. Multiple attempts may result in failed oxygenation as trauma to the laryngeal inlet caused by laryngoscope blade manipulations or blind attempts at tube passage result in bleeding, laryngospasm, and edema. Severe hypoxemia esophageal intubation, regurgitation, aspiration, bradycardia and cardiac arrest are reported.
7.2.2.2Response to difficult direct laryngoscopy (DL)
For the reasons of the danger of multiple intubation attempts, total intubation attempts should be limited. As such, the clinician should maximize the chances of success with the first, and if needed, each succeeding attempt.
Before the first attempt at laryngoscopy, a plan for difficult laryngoscopy should be mentally rehearsed, all equipment assembled, and assistants briefed on what to expect and how they can help (e.g., with immobilization, two-person BMV, cricoid pressure, external laryngeal manipulation [ELM] etc.). The position of both the patient and clinician should be optimized, and an appropriately sized blade selected. If a skeletal muscle relaxant is used, it must be given time to act.
7.2.2.3 Initial Response to difficult DL
7.2.2.4 Second and Subsequent Attempts at DL: With experience, many anesthetists or clinicians will recognize after a single attempt that successful intubation using DL is unlikely, and may choose to move on to an alternative intubation technique. Given the increasing morbidity with multiple intubation attempts, a second or subsequent attempt at DL should be undertaken only if something different can be done, for example:
A blade change need not be an automatic response to a difficult laryngoscopy situation, and should be undertaken only with a specific goal in mind. Such situations may include the following:
7.2.2.5 Moving on to an alternative, non-DL intubation technique
Following a second failed attempt at intubation, the patient should again be oxygenated with BMV. As long as mask ventilation continues to be nonproblematic, a third attempt at intubation can be considered. However, after two failed attempts at intubation using best look DL, a third attempt at laryngoscopic intubation is rarely warranted, unless a more skilled anesthetist has arrived. Rather, an alternative intubation technique should now be considered depending on the availability, the skill and experience of the anesthetist. The alternative intubation devices are scarce to none existent even in our big hospitals require focused training and the success rates will depend on the individual clinician's skill. But it is adviced that all anesthetists who regularly manage airways should have skills in using at least one alternative intubation technique.
As previously outlined, the failed airway is defined in one of two ways: failed intubation, defined simply by a failure to intubate after three attempts(can't intubate, CAN oxygenate) , one is still dealing with an oxygenated patient, or failed oxygenation failure to intubate in conjunction with a failure to oxygenate using BMV (can't intubate, CAN'T oxy-genate), a hypoxic one.
7.2.3.1 Failed Airway: Failure to intubate and/or failure to oxygenate with bag mask ventilation represent decision point in airway management that requires urgent action. There are two pathways that define the failed airway these are failed intubation and failed oxygenation
7.2.3.2 Failed Intubation is defined by the failure to intubate the patient after three attempts by an experienced clinician (i.e., can't intubate, can oxygenate). (See ANNEX -1)
i. Failure to intubate after three attempts on the part of any one clinician should be a warning sign to stop, take stock, and reassess the situation. Otherwise, “fixation error” can set in, with a harried clinician focused excessively on the intubation, while losing sight of the “bigger picture” of ensuring patient oxygenation
ii. As previously presented, multiple intubation attempts are associated with increasing morbidity. At its worst, multiple attempts could eventually cause trauma, edema, and bleeding to the extent that mask ventilation now becomes impossible.
iii. Neuromuscular blockade may have worn off, and a decision will have to be made about allowing the patient to resume spontaneous ventilation with no further doses of muscle relaxant or conversely, whether a second dose should be given.
After a third failed attempt, the patient should again be ventilated by BMV to reoxygenate and indeed, confirm that the patient can still be mask ventilated. At this point, although BMV can continue indefinitely, we espouse placing a rescue oxygenation device, in the form of an extraglottic device such as LMA. It confers a number of advantages: once placed, it generally enables easier positive pressure ventilation of the patient, often with just one hand; it delivers positive pressure ventilation from just outside the laryngeal inlet. Once oxygenation is confirmed and the situation has stabilized, definitive care should be arranged.
Note that clinical judgment should be applied to the directive to limit intubation attempts to three. For example, if a more experienced colleague has arrived, a fourth attempt may be warranted by that clinician, or similarly, if an adjunct such as a bougie has now become available, a further attempt may be undertaken.
7.2.3.3 Failed oxygenation: Failed oxygenation assumes that in addition to a failed attempt at intubation, the patient cannot be oxygenated (i.e., to SaO2of 90% or more) with BMV (i.e., can't intubate, can't oxygenate).
The inability to oxygenate the patient with mask ventilation or via an endotracheal tube is an emergency situation. The default intervention for this failed oxygenation situation is cricothyrotomy, emergency techniques designed for accessing the airway through the cricothyroid membrane. The cricothyroid membrane can be identified by first locating the thyroid cartilage and then sliding the fingers down the neck to the membrane, which lies just below. Access to the lower airway through the cricothyroid membrane can be by open surgical or percutaneous, needle-guided cannula techniques.
Before declaring a failed oxygenation situation, an aggressive response to difficult BMV should have been undertaken. As mentioned earlier, this includes an oral airway and two-person technique (Session V Figure 5.15).
In most situations, before cricothyrotomy, trying extraglottic device such as placement of laryngeal mask air way (discussed in session IV) and intubating with Combitube should be attempted. Extraglottic device (EGD) may succeed where BMV has failed for the following reasons:
EGDs may not succeed in oxygenating and ventilating the patient with pathology or obstruction at or below the cords. If EGD placement is successful in a failed oxygenation situation, cricothyrotomy can be avoided, and definitive care should be arranged. It must be emphasized, however, that in the failed oxygenation situation, the EGD placement attempt must be brief, and must not delay the onset of cricothyrotomy. In practice, this translates to a single attempt at EGD insertion while the cricothyrotomy package is being opened.
Finally, the occasional patient may present with pathology rendering airway access from above the cords obviously impossible from the outset. These patients may require a primary cricothyrotomy or tracheostomy.
7.2.4.1 The use of Combitube in difficult air way
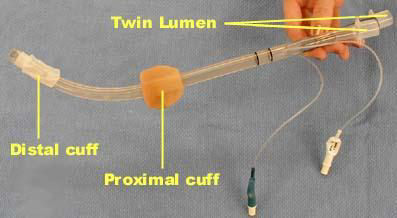
The Combitube (Figure 7.1) is a twin lumen device designed for use in emergency situations and difficult airways. It can be inserted without the need for visualization into the oropharynx, and usually enters the esophagus. It has a low volume inflatable distal cuff and a much larger proximal cuff designed to occlude the oropharynx and nasopharynx.
If the tube has entered the trachea, ventilation is achieved through the distal lumen as with a standard ETT. More commonly the device enters the esophagus and ventilation is achieved through multiple proximal apertures situated above the distal cuff. In the latter case the proximal and distal cuffs have to be inflated to prevent air from escaping through the esophagus or back out of the oropharynx and nasopharynx.
The Combitube can only be used in the adult population as no pediatric sizes are available. Complications of the Combitube include an increased incidence of sore throat, dysphagia and upper airway hematoma when compared to endotracheal intubation and LMA. Compared to intubation with an endotracheal tube under direct laryngoscopy or using the LMA, the Combitube seems to exert a more pronounced hemodynamic stress response. Although it is possible to maintain an airway with the Combitube, endotracheal intubation is the preferred method for definitively securing the airway. The available sizes are 41 Fr and 37 Fr. The original recommendations by the manufacturer is to use 41 Fr for patients taller than 5ft (152 cm) and 37 Fr for patients below that height.
6.2.4.2 Cricothyrotomy: is a procedure that involves placing a tube through an incision in the cricothyroid membrane to establish an airway for oxygenation and ventilation. Cricothyrotomy can be performed by placing a small needle or catheter (neele cricothyrotomy), a large cannula specially designed for this purpose, or surgically inserting a cuffed tube.
 |
 |
| Figure 7:2 With thumb and long finger stabilizing the thyroid cartilage, the index finger palpates the cricothyroid membrane. | Figure 7:3 Needle cricothyrotomy set-up using a large-bore IV, the barrel of a 3-cc syringe attached to the connector of a 7.0 ETT. The assembly is attached to a BVM device or oxygen source |
7.2.4.4 Tracheostomy: a surgical incision between the second and third tracheal ring to make a temporary air way so as to allow air to get to the lungs in cases of failed oxygenation. This can be done before anesthesia if there is prediction of failed intubation and oxygenation following induction of anesthesia.