2.1 Bowel obstruction or intestinal obstruction:
2. Acute Abdomen: The term acute abdomen denotes any sudden condition with chief manifestation of pain of recent onset in the abdominal area which may require urgent surgical intervention.
It is a partial or complete blockage of the intestine that keeps food or liquid from passing through from small intestine or large intestine and producing symptoms of vomiting, constipation, distension and abdominal pain.
2.1.1 Pathophysiology of intestinal obstruction
Obstruction leads to proximal dilatation of the bowel and disrupts peristalsis. Bowel above the obstruction becomes distended with fluid and gas. This stimulates excessive peristalsis producing colicky pain. As distension increases with time, blood vessels in the bowel will be stretched and narrowed impairing blood flow and leading to ischemia. Absorptive capacity of the gut decreases with a net increase of water and electrolytes secretion into the lumen. There will be increased vomiting which leads to depletion of extra cellular fluid which eventually leads to hypovolemia and dehydration. A strangulated loop dies and perforates to produce severe bacterial peritonitis which is often fatal. Grossly distended abdomen restricts diaphragmatic movement and interferes with respiration. A multiple organ failure will subsequently result if the strangulated loop is not removed.
2.1.1.1Small intestine obstruction: It causes pain, distension, emesis, and severe constipation. Volume loss, tachycardia, and electrolyte disturbances can occur from severe vomiting and the massive volumes that are sequestered (loss of fluid content in to the spaces with in the body, so that the circulating volume diminishes) in strangulated bowel (Figure 2:2). With obstruction, not only is reabsorption hindered, but intestinal fluid secretion may be increased. This effects to increase intraluminal (inside space of a tubular structure such as the inside of the intestine) pressure to exceeds and reabsorption fails. If strangulation (the constriction of the tubular structure of the body such as a segment of bowel which causes arrest of circulation in part due to compression) occurs, necrosis of bowel and bacterial proliferation contribute to rapid sequestration of fluid and colloid in the affected bowel and peritoneal cavity. Together with vomiting, this can produce marked depletion of intravascular volume and the potential for renal and cardiovascular instability.

Figure 2:1 Volvulus
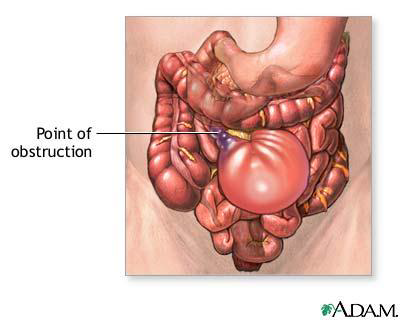
Figure2:2 Sequestration of fluid following
obstruction
2.1.1.2 Acute, large bowel obstruction: It is associated with pain, distension, vomiting, and severe constipation, although large bowel obstruction can be more insidious than small bowel obstruction and may present without pain. Large bowel obstructions result from colorectal cancer, diverticulitis (is small bulging sacs or pouches of the inner lining of the intestine that become inflamed or infected), volvulus (complete twisting of a loop of intestine), and fecal impaction. The sigmoid colon is the most frequent site of volvulus in the large bowel (Figure 2:1).
2.1.2 General management
- Decompression of the stomach (nasogastric tube)
- Fluids resuscitation to restore the circulatory state
- Early preoperative preparation and early laparatomy
- Attempt rectal tube deflation in assumed viable large bowel obstruction
- Attention to conditions in other systems (e.g., infection, renal and cardiovascular problems)
2.1.3 Anesthetic consideration
2.1.3.1 Preoperative preparation
- Full history including drugs and compliance to drug, physical examination and analysis of the preoperative investigations, the resuscitation need of the patient should be assessed.
- The clinical presentation of intestinal obstruction may vary enormously, from mild dehydration in a well nourished patient to a shocked, septic patient with severe abdominal pain and reduced conscious level.
- Patients presenting with an intra-abdominal catastrophe (acute obstruction) are often extremely unwell, with marked hypovolemia, hypoperfusion, acidosis, severe renal impairment, and sepsis. Aggressive preoperative optimization in this group of patients is often beneficial in preoperatively before rushing to operation.
- All cases will need some degree of fluid resuscitation to restore the circulating volume and adequate urine output. The majority of cases of intestinal obstruction requiring surgery are categorized as urgent (that is surgery need to be performed within 24 hours) allowing the procedure to be performed during routine operating hours with ready availability of all staffs and after resuscitation.
- The goals of pre-operative fluid management are to restore vascular and interstitial volumes and to correct electrolyte and acid-base imbalances. This will normalize systemic vascular resistance and optimize oxygen delivery. The initial choice of fluid is usually crystalloid balanced salt solutions.
- Fluid volume should be administered depending on the estimated deficit and the time available to ensure the circulatory volume before induction of anesthesia. Always use large bore IV cannula.
- Oxygen should be administered to most emergency laparotomy procedures in the preoperative period especially if hypotensive or with an oxygen saturation of less than 95% on pulse oximetry.
- Urinary catheter: start hourly measurement of urine output and use to guide fluid therapy.
- A nasogastric tube should be inserted in patients presenting with intestinal obstruction to relieve gastric distension and reduce the risk of aspiration.
- Give antibiotics where appropriate.
2.1.3.2 Intraoperative anesthetic care
- Make sure that any resuscitation measures commenced are continued up to the time of induction of anesthesia.
- Patients with GI motility disorders and those with obvious obstruction are at risk for regurgitation and aspiration during the induction and maintenance of anesthesia and postoperatively. Anesthesia should be induced using awake intubation or rapid sequence considerations.
- The technique of rapid sequence induction is explained in session 1 anesthesia consideration for emergency surgery
- Apply available monitor, take base line value and continue monitoring throughout the procedure and postoperative period.
- Have a large-bore IV connected to pressurized fluids and infusing rapidly.
- Choice of induction agent depends on cardiovascular stability. Dose should be titrated starting from low dose.
- Relaxants: suxamethonium for induction and other long acting for maintenance (Vecuronium)
- Maintenance of anesthesia depends on the patient response for available anesthetics. Oxygen, small concentration of halothane (.5 -1 vol%) or ketamine drip, titration of fentanyl 1-2 μg/kg or pethedine .25mg/kg, long acting muscle relaxant (Vecuronium .05- .1 mg/kg) can be used. Abdominal surgery requires good muscle relaxation for optimal surgical exposure making controlled ventilation an absolute necessity.
- Careful fluid management is essential for improving the outcome following major abdominal surgery. The volume of fluid administered should be the sum of hourly maintenance requirements, pre-existing deficits and ongoing losses.
- Analgesia: Fentanyl or morphine is good options. Give with induction and supplement as needed.
- Vasopressors and vagolytic should be drawn up before induction (atropine, glycopyrrolate, ephedrine and adrenaline). If hypotension persists prepare an adrenaline infusion to administer at a rate of 3 to 12 microgram per minute and dopamine 3- 10microgram perminute.
- Patient warming should be as for any laparotomy.
- Regional anesthesia is not a good choice
2.1.3.3 Postoperative care
- Awake extubation
- The highest priority is maintaining airway, breathing, and circulation
- Aggressive treatment of hypothermia, maintain blood pressure and pulse rate.
- Frequent review of postoperative fluids should be undertaken.
- Urine output should be measured hourly intra and postoperatively. If <0.5 ml/kg/h urgent review is necessary.
- Oxygen should be administered postoperatively.
- Pain should be treated in titrated dosage (morphine)