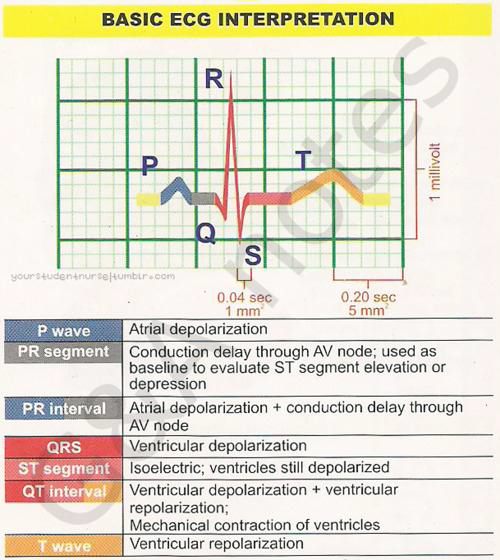
The contraction and relaxation of cardiac muscle result from the depolarization and repolarisation of myocardial cells. These electrical changes are recorded via electrodes placed on the limbs and chest wall and are transcribed on to graph paper to produce an electrocardiogram (commonly known as an (ECG).
Electrocardiogram is recorded on to standard paper travelling at a rate of 25 mm/s. The paper is divided into large squares, each measuring 5 mm wide and equivalent to 0.2 s. Each large square is five small squares in width, and each small square is 1 mm wide and equivalent to 0.04 s.
The arrangement of the leads produces the following anatomical relationships:
Rate
The term tachycardia is used to describe a heart rate greater than 100 beats/min. A bradycardia is defined as a rate less than 60 beats/min (or < 50 beats/min during sleep).
Rhythm
To assess the cardiac rhythm accurately, a prolonged recording from one lead is used to provide a rhythm strip. Lead II, which usually gives a good view of the P wave, is most commonly used to record the rhythm strip. The term sinus rhythm is used when the rhythm originates in the sinus node and conducts to the ventricles. Young, athletic people may display various other rhythms, particularly during sleep. Sinus arrhythmia is the variation in the heart rate that occurs during inspiration and expiration.
Cardinal features of sinus rhythm
Sinus bradycardia- heart rate <60beats/min
Sinus bradycardia is common in normal individuals during sleep and in those with high vagal tone, such as athletes and young healthy adults. The electrocardiogram shows a P wave before every QRS complex, with a normal P wave axis (that is, upright P wave in lead II). The PR interval is at least 0.12 s. The commonest pathological cause of sinus bradycardia is acute myocardial infarction. Sinus bradycardia is particularly associated with inferior myocardial infarction as the inferior myocardial wall and the sinoatrial and atrioventricular nodes are usually all supplied by the right coronary artery.

Many patients tolerate heart rates of 40 beats/min surprisingly well, but at lower rates symptoms are likely to include dizziness, near syncope, syncope, ischaemic chest pain, and hypoxic seizures
Pathological causes of sinus bradycardia
Sinus tachycardia- heart rate 150-200beats/min
Sinus tachycardia is usually a physiological response but may be precipitated by sympathomimetic drugs or endocrine disturbances. The rate 150- 200 beats/min in adults. The rate increases gradually and may show beat to beat variation. Each P wave is followed by a QRS complex. P wave morphology and axis are normal, although the height of the P wave may increase with the heart rate and the PR interval will shorten. With a fast tachycardia the P wave may become lost in the preceding T wave. Recognition of the underlying cause usually makes diagnosis of sinus tachycardia easy. A persistent tachycardia in the absence of an obvious underlying cause should prompt consideration of atrial flutter or atrial tachycardia.

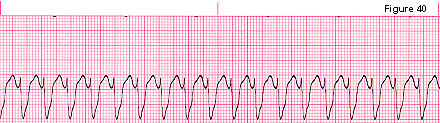
Ventricular tachycardia
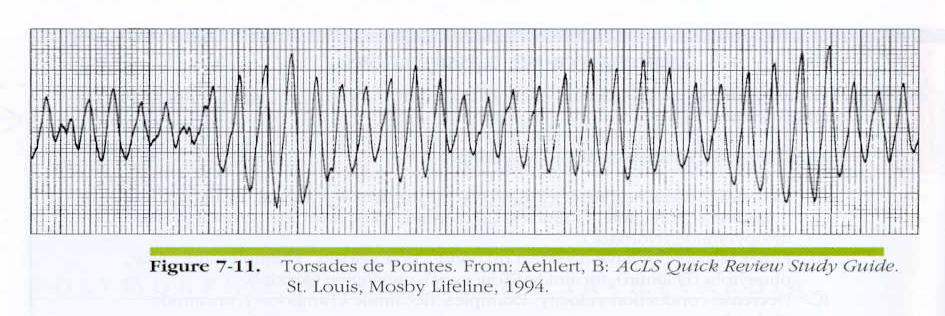
Ventricular tachycardia is described as monomorphic when the QRS complexes have the same general appearance and polymorphic if there is wide beat to beat variation in QRS morphology. Monomorphic ventricular tachycardia is the commonest form of sustained ventricular tachycardia